Get active
7 easy ways to increase your steps count

BHF Senior Cardiac Nurse Regina Giblin explains that intermittent claudication is the medical term for pain in the legs when walking. It's a sign of peripheral arterial disease (PAD), which is also known as peripheral vascular disease (PVD).


Many people mistakenly think having painful legs is just part of growing older. But if you do not have hip, knee or joint problems then there's no reason why you should have sore legs.
So, if you start experiencing pain in your legs when walking that goes away with rest, you could have intermittent claudication.
This is the medical term used to describe this type of pain, which is the main symptom of peripheral arterial disease (PAD), also known as peripheral vascular disease (PVD).
Intermittent claudication is usually felt as a cramp or pain in the leg muscles when you’re walking. It can range from mild to severe and is relieved by rest within 10 minutes.
The pain most commonly affects the calves, rather than the thigh, buttocks or hips. It can be in both legs at the same time, or worse in 1 leg.
Other symptoms of intermittent claudication include fatigue and discomfort, and some people describe the pain as aching or burning.
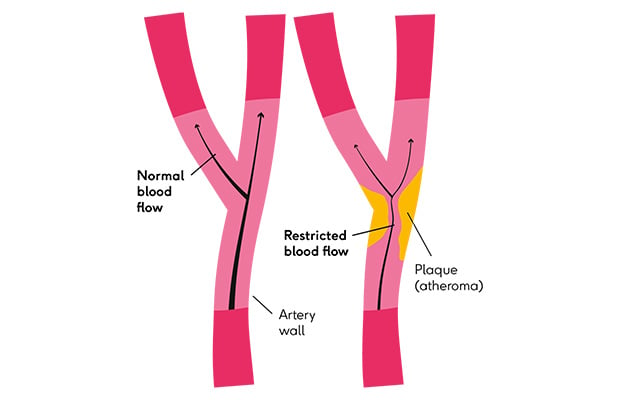
Intermittent claudication is the main symptom of PAD, which is a circulatory system condition that happens when fatty material builds up (atherosclerosis) inside the arteries of the legs. These fatty plaques are made up of cholesterol and other waste products.
These fatty plaques can cause pain when you walk because they narrow the arteries, preventing enough oxygen-rich blood from getting to your leg muscles, causing the cramping-like pain.
Atherosclerosis in the legs, leading to PAD and intermittent claudication, is the same as the atherosclerosis in your coronary arteries that leads to coronary heart disease and chest pain (angina), which are both cardiovascular diseases.
The 2 conditions share the same risk factors, such as having an unhealthy lifestyle and conditions like high blood pressure (hypertension) and high cholesterol (hypercholesteraemia).
PAD and coronary heart disease both increase the risk of heart attack and stroke.
In fact, research suggests having PAD increases your risk of dying from cardiovascular disease by up to 6 times compared to those who do not have PAD.
There are also other risk factors that increase the likelihood you will develop PAD and experience intermittent claudication. These include:
As well as intermittent claudication other symptoms of PAD include:
Symptoms of PAD usually develop slowly over time. At the early stages, you may have no symptoms.
But if your symptoms develop quickly, or get suddenly worse, you could require emergency treatment. If this happens call NHS 111 or 999.
If your GP suspects the pain in your legs when you walk is intermittent claudication, they will perform some diagnostic tests for PAD.
They will physically examine your legs and measure blood pressure in your ankle, which they will compare with the blood pressure in your arm.
This is called the ankle brachial pressure index (ABI). If there is a difference in blood pressure between the ankle and arm, it suggests the pain is likely being caused by intermittent claudication and you have PAD.

Some GP surgeries will also use a doppler scan to check how well blood is flowing in your legs. The scan picks up a swooshing sound as blood moves through the legs to the ankles.
If your GP suspects you have PAD, they will assess your risk of heart attack and stroke too. They will do this by checking your blood pressure and cholesterol levels, finding out if you smoke and how healthy your lifestyle is.
If it’s difficult to diagnose PAD, or if the circulation to your legs is very poor and you have ulcers or gangrene, your GP will refer you to hospital for an MRI of your legs.
Treatment for intermittent claudication aims to improve the blood flow to your legs so enough oxygen-rich blood gets to your leg muscles when you walk.
The NHS recommends taking part in a supervised exercise programme for 2 hours a week over 3 months to boost blood flow to the legs.
During this programme, you will be encouraged to exercise to the point where you feel the intermittent claudication pain. The aim is to increase the distance you can walk and the length of time you can walk before you feel any pain.
If a supervised programme is unavailable a healthcare professional will support you to exercise by yourself at home.
You will also be encouraged to adopt a healthy lifestyle, which may include quitting smoking, eating a healthy, balanced diet that’s low in saturated fat and salt.
If you are found to be at risk of heart attack and stroke, your GP may prescribe medicines to lower high blood pressure, high cholesterol, and high blood sugar levels if you have diabetes.
By treating these risk factors to reduce your overall risk of heart attack and stroke, your doctor will also be treating your PAD, which as explained above is the underlying cause of intermittent claudication.

If exercise and a healthy lifestyle fail to alleviate your leg pain, your medical team may suggest a more aggressive treatment plan.
If the blood supply to your leg is severely affected, a surgical procedure called an angioplasty to open-up a blocked artery in your leg may be necessary.
Some people need a bypass operation to redirect the blood around a partially or fully blocked artery so blood can flow around the legs properly.
If your leg pain does not improve with exercise, and you do not want to have surgery, then speak to your specialist medical team about other treatment options.
Chronic limb-threatening ischaemia happens when so little blood is flowing to the legs and foot you’re in constant pain and may have ulcers or gangrene. This is the end stage of PAD and doctors may need to amputate the leg or foot.
British Heart Foundation (BHF) is funding science into PAD, including research at King’s College London and St Thomas’ Hospital into an imaging technique that can see if surgery to a PAD-affected limb has been successful.
The same researchers are looking at how they can encourage new blood vessels to grow to replace blocked arteries in PAD.