Heart attack treatment - CvLPRIT
Should all narrowed coronary arteries be reopened during angioplasty for STEMI heart attack?
The clinical question
A STEMI heart attack is caused by a complete blockage in one of the coronary arteries that supply blood to the heart. This type of heart attack is usually treated with emergency procedure to reopen the blocked 'culprit' artery. This is known as an angioplasty (or primary percutaneous intervention, PCI). However, about half of these patients have additional narrowed areas in other coronary arteries.
Doctors were unclear whether they should treat these partial blockages during the emergency angioplasty procedure. Some believe that opening other narrowed arteries might reduce the risk of having another heart attack. But this comes at the potential cost of a more complicated procedure, which could be a risk for the patient.
So Professor Anthony Gershlick and his team at the University of Leicester designed the BHF-funded ‘Complete Versus Lesion-only Primary PCI Pilot Study’ (CvLPRIT). The aim was to find out whether only the ‘culprit artery’ should be treated during emergency PCI, or whether other narrowed arteries should also be opened prior to discharge from hospital.
What did the study involve?
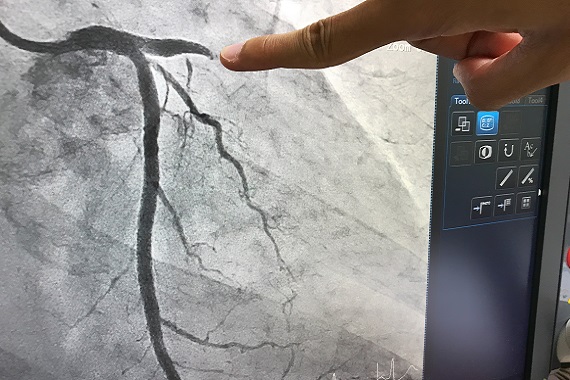
From 2011 to 2014, the research team screened 850 people experiencing a STEMI heart attack. Their doctors performed an angiogram, an X-ray procedure that allows doctors to visualise the coronary arteries to identify blocked or narrowed areas. 296 patients were found to have partial blockages in one or more of the vessels supplying their heart, in addition to the ‘culprit’ blockage that directly caused their heart attack. Participants in the trial either:
- Had a procedure to reopen only the culprit artery.
- Had the culprit artery plus other significant partial blockages reopened.
For most patients in the second group, the doctors could treat all affected coronary arteries during one procedure. If not, further procedures were carried out during the patient’s initial admission to hospital.
What did the study show?
At 1 year after their treatment:
- Participants who had partially blocked vessels opened in addition to the ‘culprit’ artery were more likely to have survived.
- These participants were also less likely to have experienced further serious heart-related complications.
Longer term follow up showed that these beneficial effects were still present up to 7 years after their admission to hospital. As a result, the research team believe this ‘complete’ treatment method gives better outcomes for patients, while being more cost effective for the NHS.
Why is the study important?
Professor Gershlick presented the results of CvLPRIT at the 2014 European Society of Cardiology Conference in Barcelona. He said: “We found that complete revascularisation leads to a 55% reduction in overall mortality and risk of major adverse cardiac events at 12 months."
This mirrors what was found in other studies, and tells us that we should at least be thinking about treating our patients for complete revascularisation during their initial admission to hospital.
Professor Anthony Gershlick, Chief Investigator, CvLPRIT
The results of CvLPRIT contributed to a change in current European and USA guidelines for the treatment of STEMI heart attack. Previously, opening additional arteries as well as the culprit artery was not recommended. These guidelines now suggest that, if patients have additional partial blockages in blood flow to their heart, their doctor should consider reopening these as well prior to discharging them from hospital.
Study details
"Complete versus lesion-only primary PCI pilot (CVLPRI-t)"
Award reference: SP/10/001/28194
Principal Investigator: Professor Anthony Gershlick, University of Leicester
Publication details
Gershlick AH, Khan JN, Kelly DJ, et al. Randomized trial of complete versus lesion-only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease: the CvLPRIT trial. J Am Coll Cardiol. 2015;65(10):963-72.